








Relapse common on road to recovery






Patricia Kearns' son was 47 when he died of a heroin overdose in Baltimore nearly four years ago.
The Lewes resident holds back tears as she explains the shame she felt, not as a mother of a heroin addict, but for being afraid to talk about it.
If you or someone you know is struggling with addiction and substance abuse, go to helpisherede.com or call 800-345-6785.
“And it's that shame that kept him from asking for help,” she said. “The call of the drug is a lot stronger than anyone can believe.”
Shortly before Patrick died, Kearns and her family had arranged for him to go to a 28-day rehab center, but he refused the help. At the time, Kearns knew her son had a problem, but she didn't know for sure that it was heroin.
“If a parent thinks their child is using, they're probably right,” she said. “It's not just the people who come from the wrong side of the road.”
Kearns said nothing is going to change about the heroin epidemic, or the hundreds of lives it claims, until enough people get involved. She said she wants to see more treatment resources in communities – including her own.
“There are no boundaries with this,” she said. “When the living can't admit there's a problem, we're not helping. I'm very concerned about people having their heads in the sand.”
She said she saw her son struggle with employment and relapses over the years, and he constantly denied there was a problem. “For a long time, you can excuse a lot of things,” she said. “I've got more questions than I'll ever have answers. I feel like there's a lost child out there and I'm still looking for him. When you love an addict, you live on the edge, but you're never, ever prepared for that call.”
User perspective: A young, white Sussex County man
By Maddy Lauria
After failing multiple drug tests during an outpatient program nearly 30 minutes from his home, a relapsed addict, who is not named to protect his privacy, frantically texts all the dealers in his phone. He's sweaty, nervous and pale. He hasn't had a fix in 24 hours.
He's white, 27, and this is at least his fifth time going through treatment and relapse. His first opiate experience: A Percocet his mother gave him when he was sick and still a teen.
“I was in love,” he said. “I started taking them regularly. Then I found out you can snort them. Then I started freebasing them. It all went downhill from there. It got really expensive, and heroin's cheaper."
He said he found a deep connection to the highs that made him feel like the sun was always shining and everything was going to be OK.
His most recent attempt to get clean started at the end of 2015 when he visited a Sussex County facility hoping to start medication-assisted treatment the same day. He was told it would be three weeks before he could get Suboxone, a combination of buprenorphine and naloxone, to help with withdrawal symptoms and cravings.
“What am I supposed to do for three weeks?” he asked.
“You can try snorting it instead,” he said a clinic worker told him. He said he didn't listen and kept shooting heroin for three weeks, until he could finally start treatment. The Suboxone strips he placed under his tongue each morning kept him clean for a while, not counting the marijuana and alcohol he was still using. He continually failed drug tests while in the program because he was still using other substances and faked sign-ins for support group meetings.
He decided he needed something stronger than Suboxone. A doctor agreed to give him Vivitrol – an extended release form of naltrexone given as a monthly shot to block the effects of opioids and heroin. He knew he wouldn't be able to use once he got the shot. He decided to get high one last time.
Because he didn't tell his doctor about the recent use, when Vivitrol was administered he was sent into an immediate, painful withdrawal. And he had no connections or support outside of the clinic.
Normally, he knew exactly what would fix the misery of diarrhea, vomiting and flu-like symptoms that come with withdrawal: More opioids. But nothing would help the Vivitrol-induced withdrawal because the shot blocks the opioids from binding with the brain and releasing the dopamine associated with the high. He tried more drugs, but the pain continued for nearly a week.
By the time he recovered, he gave up on treatment altogether and relapsed again. He hasn't heard from the clinic since.
“It's hopeless around here,” he said. “And once you're labeled as an addict, that's what you are.”
Existing resources stretched thin
As the supply and demand for heroin and illegal opioids increases, treatment resources in Delaware are finding they are increasingly overburdened.
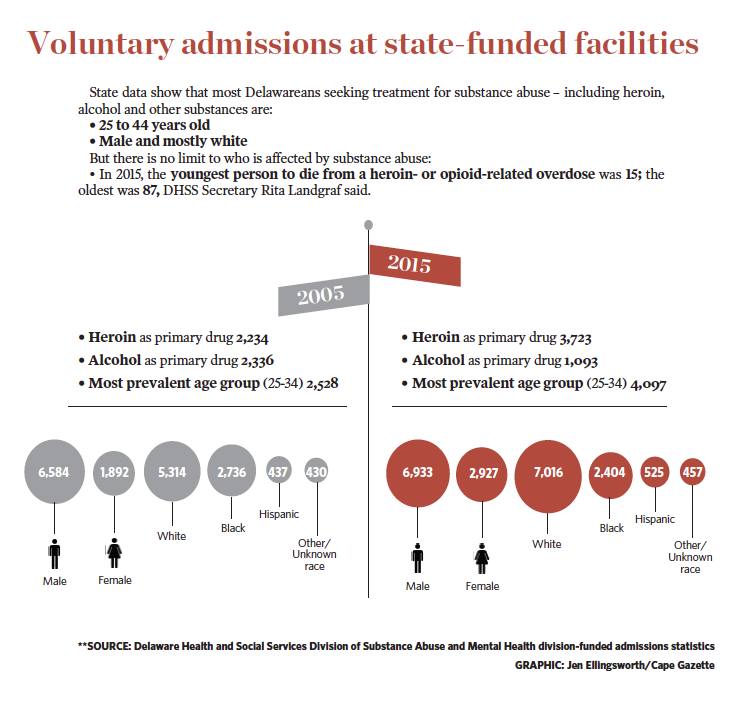
“We're limited in capacity statewide,” said state Department of Health and Social Services Secretary Rita Landgraf. “We do have a heroin epidemic, but the root cause of that heroin is addiction.”
When they finally seek treatment, about 90 percent of heroin users will relapse, so it's imperative that addicts get appropriate care quickly and close to home, Landgraf said.
Mental health treatment facilities in Delaware were strained even before the heroin epidemic flooded the First State, especially in coastal and rural Sussex County, Landgraf said, so efforts to bring more resources are like playing catch up.
When Connections Community Support Programs Inc. opened a treatment clinic in Millsboro, CEO Cathy McKay and her team of specialists expected to treat about 100 patients. Fast-forward five years, and the clinic now treats about 700. The volume of patients prompted the clinic's recent move from a small space on Route 24 to the former Delaware Hospice administrative building on Old Landing Road in Millsboro.
“The new space we have still isn't big enough,” she said. “I don't think there are enough resources right now anywhere to meet the need.”
And when Connections opened a 16-bed detox center in Harrington in fall 2015, every bed was filled on the first day. Since opening, about 70 percent of patients at the detox center have been Sussex County residents.
At Addiction Medical Solutions in Rehoboth, one of the only for-profit, cash-only outpatient facilities in the county, about 300 patients receive treatment. Nearly 50 percent of patients are 18 to 34 years old, more than 62 percent are male, 96 percent are white and most are from Sussex County, a demographics report from AMS shows.
The clinic has four or five counselors, AMS Executive Director Kaci Madison said, illustrating that Sussex County facilities suffer from a shortage of staff, caused by a combination of poor pay, aging counselors and declining interest in the field.
Madison said turnover is a common problem in mental health and substance-abuse care, creating disruption in service for clients who develop trusting connections with their counselors.
“A lot of these people already have trust issues,” she said. “We all need to work together, that's the one thing I would like to see most. Let's work as a community as a whole.”
Multifaceted care needed close to home
So what's the key to successful recovery, when an addict is ready to stop using but can't afford to move away from their southern Delaware dealers and triggers?
Addiction specialists say the answer is individualized treatment with several levels of care, from inpatient to outpatient to long-term follow up and counseling, all easily accessible in the user's community.
“People don't choose to be addicted, so they can't choose not to be addicted,” said Dr. Adam Bowman, former director of community psychiatry for Connections Community Support Programs Inc. “But we're not good at recognizing the addiction early on. Once patients are in the midst of the addiction, it has really hijacked the brain, and it's hijacked their behaviors. A multifaceted approach is needed to regain that control.”
Bowman said 5 percent to 10 percent of the population is genetically predisposed to addiction, which causes people to repeatedly and compulsively seek, use and recover from the effects of drugs or other habits, such as gambling or sex, despite the consequences. In many cases, addicts suffered trauma during childhood; beyond their addiction, they may also struggle with depression, anxiety or other mental health disorders.
Bowman said medications, such as buprenorphine or Subutex, Suboxone, methadone, and naltrexone, are tools that can regulate and normalize brain function by managing withdrawal symptoms and blocking opioids from binding with brain receptors. But the biggest challenges, with or without help from medication, are changing behaviors and habits.
“Really, it's an overall lifestyle change that they can't just do on their own,” he said. “They need professional guidance, peer support and family support to make those changes and maintain those changes.”
Because so many addicts relapse, recovery extends beyond the doors of a clinic, hospital or detox facility. Medical professionals, social workers, friends, family and employers play a role in creating communities of recovery to help addicts make new connections that don't involve using drugs.
“We know treatment works," Landgraf said. "Many people are successful in recovery. It's possible for anybody.”
But in Sussex County, few resources exist for people seeking treatment.
There are detox facilities – short-term treatment centers where addicts can get a drug out of their system, often with the help of replacement therapy such as methadone or Suboxone – in New Castle County, Kent County and surrounding states.
But not in Sussex County.
There are inpatient facilities – long-term residential rehab centers that provide detox services as well as therapy and counseling – in New Castle County and surrounding states.
But not in Sussex County.
There are partial hospitalization programs, where a patient spends the equivalent of a 40-hour work week in a facility receiving care that includes medication and therapy, in New Castle County, Kent County and surrounding states. Dover Behavioral Health runs the only one in Sussex County; staff did not respond to requests for more information.
Sussex County does have outpatient programs, which provide therapy, counseling, medication for withdrawal symptoms or maintenance and other services. Most centers are based in Seaford and Georgetown, with a few in Millsboro, Lewes and Rehoboth Beach. Sober living facilities – for many, the last step in recovery – are also scattered throughout Sussex.
Treatment barriers abound
A disconnect between the different facilities and clinics throughout the state makes it difficult to track and maintain a patient's progress, Bowman said.
“Medical records are not connected,” he said. “Getting information communicated between facilities is often disjointed and doesn't occur in a timely fashion.”
It takes 60 to 90 days to change the habits and connections associated with addiction, Bowman said. Successful recovery takes much more than a few days in detox.
“When you understand the medical nature of it, it helps you better understand what kinds of treatment options you need,” he said. “It's a chronic and relapsing brain disease. The ability to quit is not there without help.”
And when people are able to get into a program, insurance often adds another barrier, Landgraf said.
“When people are ready to engage, you need the capacity,” she said, “but many times, after they dedicate to recovery, insurance says you're medically stable and we won't pay. Then you're out on the street again.”
For addicts, insurance often stops paying when vital signs recover, even though the actual journey to recovery has just started.
“We don't do that in any other disease, that you require people to go to a less restrictive treatment,” Landgraf said. “And while that's happening, that individual is starting to truly understand the disease of addiction. They're withdrawing from the substance. They have significant cravings – they can taste it, they dream about it. And that's the person we are putting out on the street.”